[From: Everly, G. & Mitchell, 3. (1997) Critical Incident Stress Management (CISM). A New Era and Standard of Care in Crisis Intervention. Ellicott City, MD:
Chevron Publishing.]
As one would never attempt to play a round of golf with only one golf club, one would not attempt the complex task of intervention within a crisis or
disaster with only one crisis intervention technology.
As crisis intervention, generically, and CISM, specifically, represent a subspecialty within behavioral health, one should not attempt application without
adequate and specific training. CISM is not psychotherapy, nor a substitute for psychotherapy. CISM is a form of psychological "first aid”.
As noted earlier, CISM represents an integrated multicomponent crisis intervention system. This systems approach underscores the importance of using
multiple interventions combined in such a manner as to yield maximum impact to achieve the goal of crisis stabilization and symptom mitigation.
Although in evidence since 1983 (Mitchell, 1983), this concept is commonly misunderstood as evidenced by a recent article by Snelgrove (1998) who argues
that the CISD group intervention should not be a stand alone intervention. This point has, frankly, never been in contention. The CISD intervention has
always been conceived of as one component within a larger functional intervention framework. Admittedly, some of the confusion surrounding this point
was engendered by virtue of the fact that in the earlier expositions, the term CISD was used to denote the generic and overarching umbrella program/
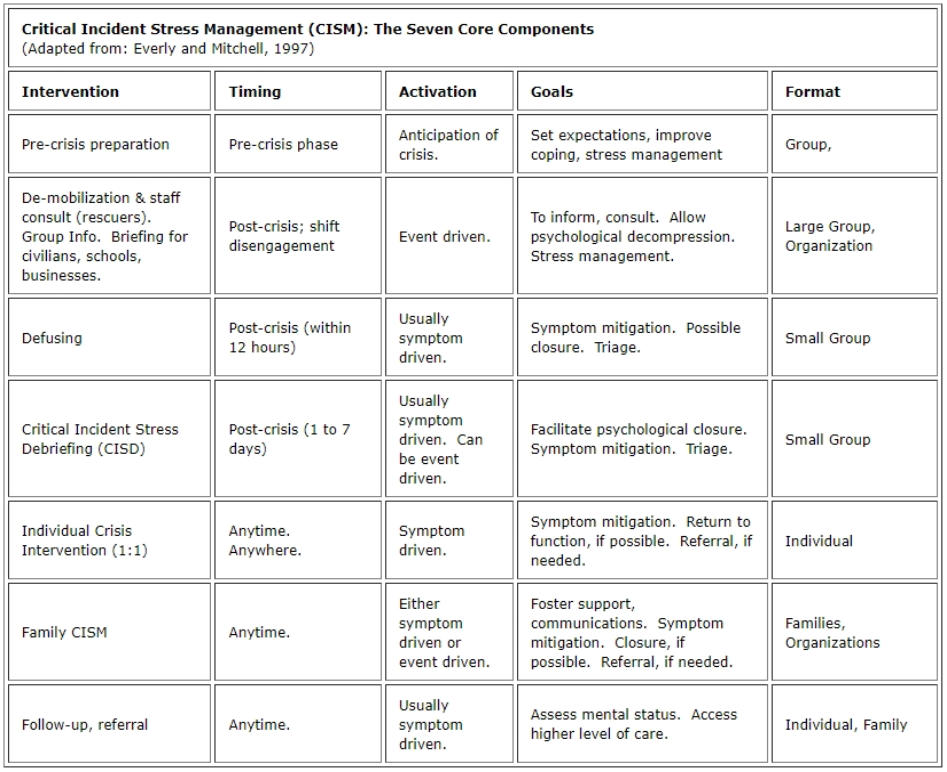
system, while the term "formal CISD" was used to denote the specific 7-phase group discussion process. The term CISM was later used to replace the
generic CISD and serve as the overarching umbrella program/ system, as noted in Table 1 (see Everly and Mitchell, 1997).
The effectiveness of CISM programs has been empirically validated through thoughtful qualitative analyses, as well as through controlled investigations,
and even meta-analyses (Everly, Boyle, & Lating, in press; Flannery, 1998; Everly & Mitchell, 1997; Everly & Boyle, 1997; Mitchell & Everly, in press; Everly,
Flannery, & Mitchell, in press; Dyregrov, 1997), unfortunately, this is a fact often overlooked (e.g. see Snelgrove, 1998).
Similarly, there is a misconception that evidence exists to suggest that CISD/ CISM has proven harmful to its recipients (e.g. see Snelgrove, 1998), this is a
misrepresentation of the extant data. There is no extant evidence to argue that the "Mitchell model" CISD, or the CISM system, has proven harmful! The
investigations that are frequently cited to suggest such an adverse effect simply did not use the CISD or CISM system as prescribed, a fact that is too often
ignored (e.g. see Snelgrove, 1998).
In sum, no one CISM intervention is designed to stand alone, not even the widely used CISD. Efforts to implement and evaluate CISM must be
programmatic, not unidimensional (Mitchell & Everly, in press). While the CISM approach to crisis intervention is continuing to evolve, as should any
worthwhile endeavor, current investigations have clearly demonstrated its value as a tool to reduce human suffering. Future research should focus upon
ways in which the CISM process can be made even more effective to those in crisis.
While the roots of CISM can be found in the emergency services professions dating back to the late 1970s, CISM is now becoming a "standard of care" in
many schools, communities, and organizations well outside the field of emergency services (Everly & Mitchell, 1997).
References
Dyregrov, A. (1997). The process of psychological debriefing. Journal of Traumatic Stress, 10, 589-604.
Everly, G.S., Boyle, S. & Lating, J. (in press). The effectiveness of psychological debriefings in vicarious trauma: A meta-analysis. Stress Medicine.
Everly, G.S. & Boyle, S. (1997, April). CISD: A meta-analysis. Paper presented to the 4th World Congress on Stress, Trauma, and Coping in the Emergency
Services Professions. Baltimore, MD.
Everly, G.S. & Mitchell, J.T. (1997). Critical Incident Stress Management (CISM): A New Era and Standard of Care in Crisis Intervention. Ellicott City, MD:
Chevron.
Everly, 0., Flannery, R., & Mitchell, J. (in press). CISM: A review of literature. Aggression and Violent Behavior: A Review Journal.
Flannery, R.B. (1998). The Assaulted Staff Action Program: Coping with the psychological aftermath of violence. Ellicott City, MD: Chevron Publishing.
Mitchell,
J.T. (1983). When disaster strikes...The critical incident stress debriefing. Journal of Emergency Medical Services, 13 (11), 49-52.
Mitchell, J. T. & Everly, G.S. (in press). CISM and CISD: Evolution, effects and outcomes. In B. Raphael & J. Wilson (Eds.). Psychological Debriefing.
Mitchell, J.T. & Everly, 0.5. (1996). Critical Incident Stress Debriefing: An Operations Manual. Ellicott City, MD: Chevron.
Snelgrove, T. (1998). Debriefing under fire. Trauma Lines, 3 (2), 3, 11.




Michigan Crisis Response Association, Inc. - 2023


[From: Everly, G. & Mitchell, 3. (1997) Critical Incident Stress
Management (CISM). A New Era and Standard of Care in Crisis
Intervention. Ellicott City, MD: Chevron Publishing.]
As one would never attempt to play a round of golf with only one
golf club, one would not attempt the complex task of intervention
within a crisis or disaster with only one crisis intervention
technology.
As crisis intervention, generically, and CISM, specifically,
represent a subspecialty within behavioral health, one should not
attempt application without adequate and specific training.
CISM is not psychotherapy, nor a substitute for psychotherapy.
CISM is a form of psychological "first aid”.
As noted earlier, CISM represents an integrated multicomponent
crisis intervention system. This systems approach underscores
the importance of using multiple interventions combined in such
a manner as to yield maximum impact to achieve the goal of
crisis stabilization and symptom mitigation. Although in
evidence since 1983 (Mitchell, 1983), this concept is commonly
misunderstood as evidenced by a recent article by Snelgrove
(1998) who argues that the CISD group intervention should not
be a stand alone intervention. This point has, frankly, never been
in contention. The CISD intervention has always been conceived
of as one component within a larger functional intervention
framework. Admittedly, some of the confusion surrounding this
point was engendered by virtue of the fact that in the earlier
expositions, the term CISD was used to denote the generic and
overarching umbrella program/ system, while the term "formal
CISD" was used to denote the specific 7-phase group discussion
process. The term CISM was later used to replace the generic
CISD and serve as the overarching umbrella program/ system, as
noted in Table 1 (see Everly and Mitchell, 1997).
The effectiveness of CISM programs has been empirically
validated through thoughtful qualitative analyses, as well as
through controlled investigations, and even meta-analyses
(Everly, Boyle, & Lating, in press; Flannery, 1998; Everly & Mitchell,
1997; Everly & Boyle, 1997; Mitchell & Everly, in press; Everly,
Flannery, & Mitchell, in press; Dyregrov, 1997), unfortunately, this
is a fact often overlooked (e.g. see Snelgrove, 1998).
Similarly, there is a misconception that evidence exists to suggest
that CISD/ CISM has proven harmful to its recipients (e.g. see
Snelgrove, 1998), this is a misrepresentation of the extant data.
There is no extant evidence to argue that the "Mitchell model"
CISD, or the CISM system, has proven harmful! The investigations
that are frequently cited to suggest such an adverse effect simply
did not use the CISD or CISM system as prescribed, a fact that is
too often ignored (e.g. see Snelgrove, 1998).
In sum, no one CISM intervention is designed to stand alone, not
even the widely used CISD. Efforts to implement and evaluate
CISM must be programmatic, not unidimensional (Mitchell &
Everly, in press). While the CISM approach to crisis intervention is
continuing to evolve, as should any worthwhile endeavor, current
investigations have clearly demonstrated its value as a tool to
reduce human suffering. Future research should focus upon
ways in which the CISM process can be made even more effective
to those in crisis.
While the roots of CISM can be found in the emergency services
professions dating back to the late 1970s, CISM is now becoming
a "standard of care" in many schools, communities, and
organizations well outside the field of emergency services (Everly
& Mitchell, 1997).
References
Dyregrov, A. (1997). The process of psychological debriefing.
Journal of Traumatic Stress, 10, 589-604.
Everly, G.S., Boyle, S. & Lating, J. (in press). The effectiveness of
psychological debriefings in vicarious trauma: A meta-analysis.
Stress Medicine.
Everly, G.S. & Boyle, S. (1997, April). CISD: A meta-analysis.
Paper presented to the 4th World Congress on Stress, Trauma,
and Coping in the Emergency Services Professions. Baltimore,
MD.
Everly, G.S. & Mitchell, J.T. (1997). Critical Incident Stress
Management (CISM): A New Era and Standard of Care in Crisis
Intervention. Ellicott City, MD: Chevron.
Everly, 0., Flannery, R., & Mitchell, J. (in press). CISM: A review of
literature. Aggression and Violent Behavior: A Review Journal.
Flannery, R.B. (1998). The Assaulted Staff Action Program: Coping
with the psychological aftermath of violence. Ellicott City, MD:
Chevron Publishing. Mitchell,
J.T. (1983). When disaster strikes...The critical incident stress
debriefing. Journal of Emergency Medical Services, 13 (11), 49-
52.
Mitchell, J. T. & Everly, G.S. (in press). CISM and CISD: Evolution,
effects and outcomes. In B. Raphael & J. Wilson (Eds.).
Psychological Debriefing.
Mitchell, J.T. & Everly, 0.5. (1996). Critical Incident Stress
Debriefing: An Operations Manual. Ellicott City, MD: Chevron.
Snelgrove, T. (1998). Debriefing under fire. Trauma Lines, 3 (2),
3, 11.